
腹膜假黏液瘤(pseudomyxoma peritonei,PMP)是少见的一种以胶冻样黏液聚集和伴有低级黏蛋白上皮构成的腹膜浸润的临床综合征[1-3],女性患者可起源于卵巢[4],病理分型是PMP患者生存期及死亡率的独立影响因素[5], 可分为低级别和高级别两种类型[6]。

腹膜假黏液瘤
临床资料
患者,女,83岁,以“腹部肿物进行性增大4年余”为主诉于2015年11月收入院,查体示全腹膨隆,肿物占据全腹,上至剑突,下至耻骨联合,双侧至双侧腋前线,隆起明显。腹软,全腹深压痛,腹部叩诊呈浊音。血生化检查示CEA(癌胚抗原)5.12 ng/ml↑, CA125(糖类抗原12-5)88.9 u/ml↑。查全腹增强CT提示:腹腔和盆腔见巨大囊实性肿物,最大截面大小303*233mm。肿块腹腔部分以囊性为著,其内可见分隔及多发乳头状突起,乳头状突起大者密度不均,部分分隔及突起可见钙化;肿块盆腔部分以实性成分主;增强扫描囊性成分未见明显强化,实性部分、分隔可见轻度强化,突起可见明显强化,子宫及附件显示不清。肝脏大小形态正常,脾脏不大。腹膜后淋巴结未见增大。增强CT所示如图1-4。增强CT诊断:腹盆腔占位性病变,首先考虑为卵巢来源,囊腺癌可能性大。


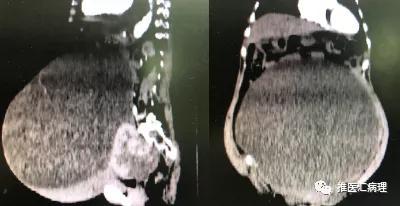
图1-4增强CT示:肿物巨大,占据整个腹腔和盆腔
因腹部肿物严重压迫周围脏器,遂给予患者于2015-11-25行腹腔肿物切除术,手术记录:全麻生效后常规消毒铺巾,取下腹部绕脐切口,长约25cm,依次切开入腹,探查见肿物大小约35cm*30cm*25cm,边界清,包膜完整,肿物呈蒂状与左侧附件区相连,肿物似来源于左侧卵巢。分次钳夹、离断、4号线缝扎肿物与卵巢相连部位,完整切除肿物。因肿物巨大,肿物切除后可能因腹腔压力聚变导致全身脏器血流动力学变化,术后给予患者于重症监护室治疗。术后查看标本:大小约35cm*30cm*25cm,包膜完整,肿物质量约15kg。剖开标本见肿物内容物为褐色液体,部分囊内壁呈菜花样及腐肉样变化。病理大体检查:送检物大部分呈囊性,大小18*20*8cm,已剖开,外壁附着一实性肿物,大小14*13*6cm,灰白,胶冻状,多结节样,内壁附着3枚结节,最大径分别为5cm-1.5cm,切面灰白,胶冻状,壁厚0.1-0.3cm,上附咖啡色物,疑为陈旧性出血,局部囊壁增厚至1.5cm,切面呈胶冻状。镜下所见如图5。病理诊断:(腹腔肿物)低级别腹膜假黏液瘤。
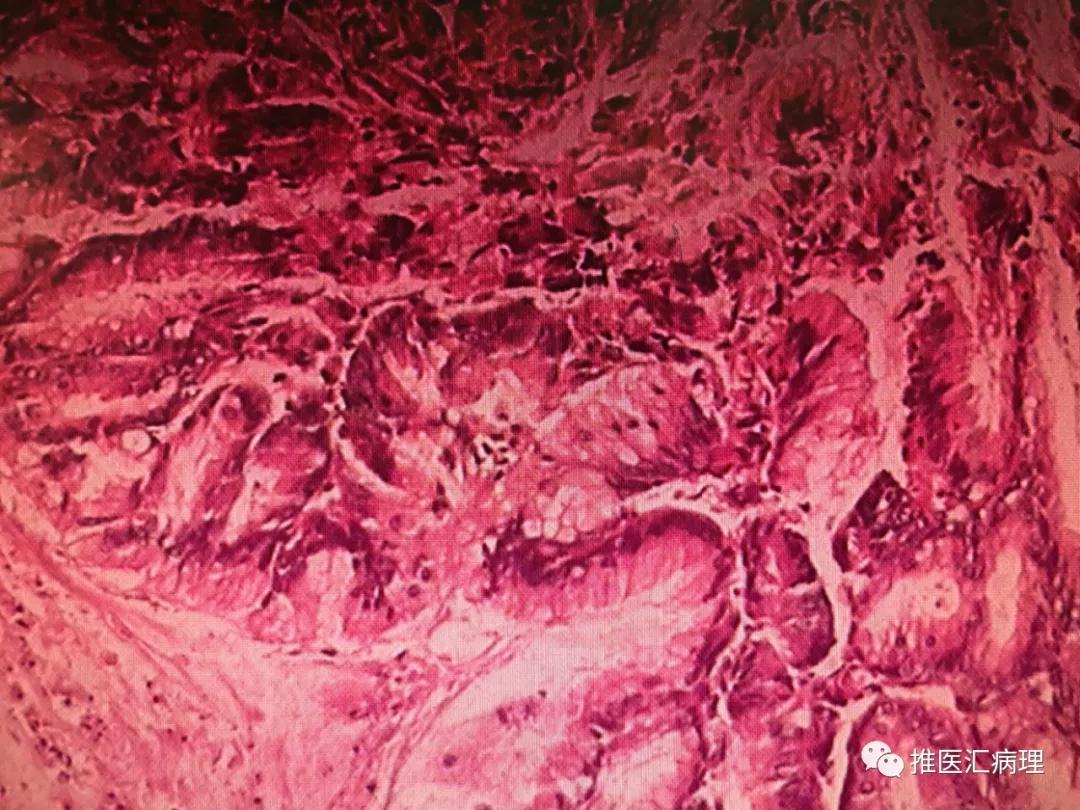
图5镜下:囊壁呈多房状,内衬单层柱状粘液上皮
讨论
腹膜假黏液瘤是以黏液外分泌细胞在腹膜种植而导致腹膜腔内大量胶冻状黏液腹水的特征性疾病[7],黏液性腹水和肿瘤细胞两者缺一不可[8]。该病的首次报道在1884年,是一例来源于阑尾的腹膜假黏液瘤,之后报道有来源于直肠[9]、胰腺[10]、胃[11]、胆管[12]甚至腹腔外器官[13-16],而卵巢来源的多为继发性[17],本文报道的该病例原发性来源于卵巢的腹膜假黏液瘤实属罕见。该病例患者腹膜假黏液瘤生长迅速,并且巨大,蔓延至整个腹腔和盆腔,其快速的生长蔓延方式,考虑是假黏液瘤经人体解剖结构间隙进行腹腔内扩散[18],借助重力作用广泛累及盆腔,当假黏液瘤破裂也可种植于盆腔和其它腹腔部位发生重新再分配现象[19-20]。根据腹膜假黏液瘤的临床发展过程及组织病理学表现,可将腹膜假黏液瘤分为良性(Disseminated peritoneal adenomucinosis,DPAM)、中间型和恶性(Peritoneal mucinous carcinomatosis,PMCA)[21]。本文报道的患者,入院肿瘤相关抗原提示CEA和CA125均升高,患者腹腔占位在短时间内迅速生长,结合术中所见及术后病理回报结果,考虑该病例的腹膜假黏液瘤为PMCA。为增加患者生存期,术中给予患者完整切除原发病灶及肉眼能见到的所有黏液囊包和黏液肿块,并细致的剥离肠管的浆膜和腹部实质脏器的被膜。患者从2015年手术至今已经随访四年,患者仍然存活并且未发现肿瘤复发。
经过对该患者的治疗,总结腹膜假黏液瘤的治疗经验是,术中探查黏液中是否含有肿瘤细胞,术中判断病灶对局部结构是否形成破坏,以及术中评估病变的累积范围,是预测腹膜假黏液瘤预后的重要因素[22-23],手术切除的彻底程度决定术后患者的生存时间和术后肿瘤复发时间,通过彻底的清除肉眼可见的假黏液瘤病灶,能够显著延缓肿瘤复发,延长患者生存时间,提高患者生存质量。
参考文献
[1]Rymer B,Forsythe RO,Husada G,Mucocoele and mucinous tumour of the appendix:A review of the literature.Int J Surg,2015,18:132-135.
[2]Smeenk RM,Velthuysn ML,Verwaal VJ,et al.Appendiceal neoplasms and pseudomyxoma peritonei:a population based study.Eur Surg Oncol,2008,34(2):196-201.
[3]Chauhan A,Patodi N, Ahmed M.A rare cause of ascites:pseudomyxoma peritonei and a review of the literature.Clin Case Rep,2015,3(3):156-159.
[4]van Ruth S,Acherman YI,van de Vijver MJ,et al.Pseudomyxoma peritonei:a review of 62 cases.Eur J Surg Oncol,2003,29:682-688.
[5]Fred T.Bosman,Fatima Carneiro,Ralph H.Hruban,et al.WHO Classification of Tumours of the Digestive system,2012,313-324.
[6]Bosman FT,Cameiro F,Hruban RH,et al.WHO classification of tumours of the digestive system [M]. Lyon: IARC,2010,417.
[7]Mann WJ Jr,Chumas J,et al.The management of pseudomyxoma peritonei[J].Cancer, 1990,66;1636-40.
[8]Holder P ,Fehir KM,Schwartz MR,et.al.Primary mucinous cystadenocarinoma a of the appendix with pseudomyxoma peritonei manifested manifested as a splenic mass.South Med J,1989,82:1029.
[9]Costa MJ.Pseudomyxoma peritonei.histologic predictors of patient survival [J].Arch Pathc Lab Med,1994,118:1215-19.
[10]Chejfrc J,Rieker WJ,jabalokow VR,et al.Pseudomyxoma peritonei associated with colloid carcinoma of the pancreas[J].
[11]Ikejii A,Anai H,Kitamura K,et al.Pseudomyxoma peritonei concomitant with early gastric cancer:report of a case[J].Surg Today,1996,16:80-2.
[12]Young RH,Scully RE.Ovarian metastases from carcinoma of the gallbladder and extahepatic bile ducts simulating primary tumors of the ovary.A report os six case[J].Int J grnecol pathol,1990,9:60-72.
[13]Kurita M,Komastu H,Hata y,et al.Pseudomyxoma peritonei due to adenocarcinoma of the lung:case report[J].J Gastroenterol,1994,29:344-8.
[14]Hawes D,Robinson R,Wira R.Pseudomyxoma peritonei from metastatic colloid carcinoma of the breast[J].Gastrointest Radiol,1991,16:80-2.
[15]Mccarthy JH,Aga R.A fallopian tube lesion of borderline malignancy associated with pseudomyxoma peritone[J].Histopathology,1998,13:233-5.
[16]Friedmann W,M,Minguillon C,Wessel J,et al.Pseudomyxoma peritonei durch en troliferierendes muzinoses Adeonm der Fimbrienschleimhau[J].Geburtshilfe Frauenheilkd,1990,50:579-80.
[17]Ronnett BM,Kurman RJ,Zahn CM,et al.Pseudomyxoma peritonei in women a clinicopathologic analysis of 30 case with emphasis on site of origin prognosis,and relationship to ovarian mucinous tumors of low malignant potential[J].Hum Pathol,1995,26:509-24.
[18]Chuaqui RF,Zhuang Z,Emmert-Buck MR,et al.Genetic analysis of synchronous mucinous tumors of the ovary and appendix[J].Hum Pathol,1996,27(2):165-171.
[19]Sugarbaker PH.Pseudomyxoma peritonei.A cancer whose biology is characterized by a redistribution phenomenon[J].Ann Surg,1994,219(2):112-119.
[20]Sugarbaker PH. Observations concerning cancer spread within the peritoneal cavity and concepts supporting an ordered pathophysiology[J]. Cancer Treat Res,1996,82:79-100.
[21]Bechtold RE,Chen MYM,Loggie BW,et al.CT appearance of disseminated peritoneal adenomucinosis[J].Abdom Imaging,2001,26(4):406.
[22]Witkamp AJ, de Bree E, Kaag MM, et al. Extensive surgical cytoreduction and intraoperative hyperthermic intraperitoneal chemotherapy in patients with pseudomyxoma peritonei[J]. Br J Surg,2001,88(3):458-463
[23]Schmidt U, Dahlke MH, Klempnauer J, et al. Perioperative morbidity and quality of life in long-term survivors following cytoreductive surgery and hyperthermic intraperitoneal chemotherapy[J]. Eur J Surg Oncol,2005, 31(1):53-58.